Alvez_48
Well-known member
Your verbal gymnastics on this issue are certainly impressive - Nadia Comaneci has got nothing on you!
For the past few weeks you've been claiming that Covid-19 deaths are being over-reported, despite being presented with evidence to the contrary, as doctors have been advised to use their clinical judgement when certifying deaths in the absence of a test result. Now you appear to have perfomed a volte-face and are claiming that the very same evidence you were informed about is, in fact, proof that the lockdown is causing significant excess deaths from other causes.
The simple fact is that we don't know. Unless the ONS changes its timetable, we won't see the data for causes of death until next year. Only then will we be able to determine whether there has been a spike in, say, heart attacks (which could possibly be lockdown related) or whether there's been a significant increase in other lower respiratory illnesses (which may be more suggestive of under-reporting of Covid-19).
Incidentally, I'm not advocating eternal lockdown, as clearly we can't simply cocoon ourselves until there is an effective vaccine (which may or may not happen). But the lockdown was necessary to buy us some time, in order that the NHS could cope with numbers and that we can try and put a properly resourced contact tracing and mass testing system in place, which is the only realistic way to try and manage this epidemic for the foreseeable future and what the government should have concentrated on in the first place.
I'm not volte facing anything those 2 things aren't mutually exclusive.
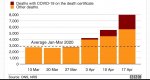
See below image might explain it more clearly.